
What motivated you to explore how cancer cells develop resistance to treatments like cisplatin, and how did this research direction evolve?
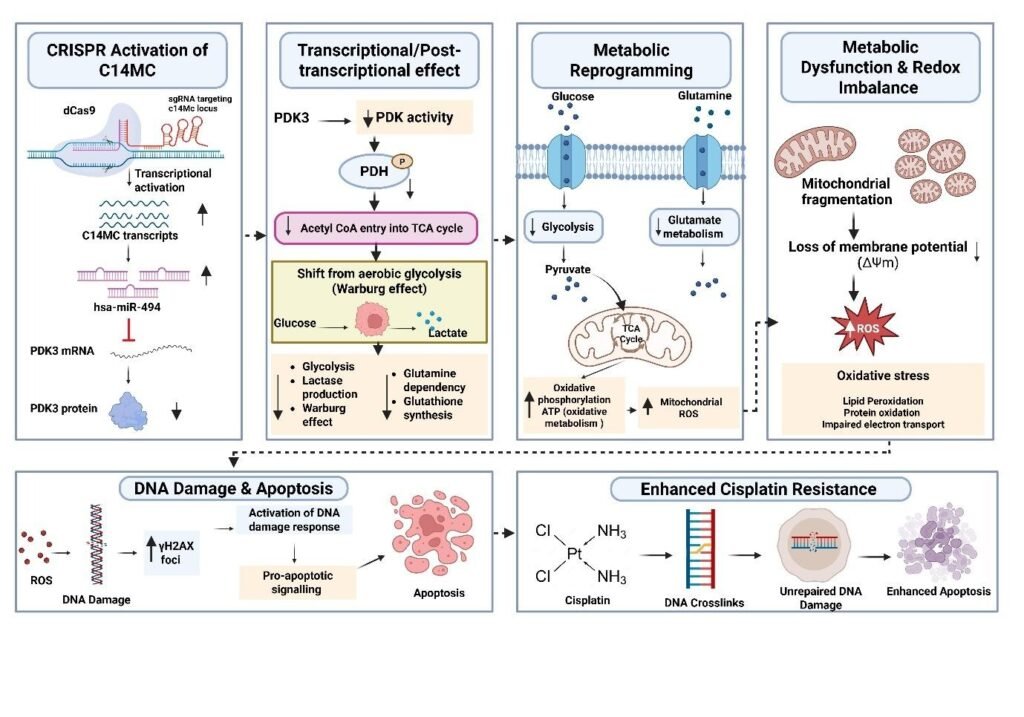
Cisplatin is a DNA-damaging agent that is commonly used as the standard of care for treating locally advanced and metastatic cervical cancer. It is usually combined with radiation to improve treatment effectiveness. Although effective, a substantial proportion of patients develop resistance to cisplatin, showing resistance and recurrence. Treatment of recurrent cases is costly and is associated with poor clinical outcomes. Our research on cervical cancer and cisplatin revealed that the structural, functional and biochemical changes in mitochondria occurred in resistant cells. More specifically, the glucose uptake, lactate production and reactive oxygen species (ROS) levels significantly differed between the resistant and sensitive populations. In addition, we also observed that the activation of the chromosome 14 miRNA cluster sensitized cervical cancer cells to cisplatin, with simultaneous changes in cellular properties, notably metabolic changes. Our experiments suggested that changes in the genome and epigenome and associated metabolomic reprogramming may play critical roles in cisplatin resistance and that targeting these changes may be used to reverse cisplatin resistance. Using microRNA sequencing, we revealed that a cluster of miRNAs on chromosome 14 was consistently downregulated in resistant cells. One of their key targets was PDK3. This discovery connected two previously separate fields: noncoding RNA biology and metabolic reprogramming. Research has evolved from epigenetics to metabolism to regulatory RNA networks, and this integrated view has opened an entirely new therapeutic window.
In simple terms, what does “metabolic reprogramming” mean, and why is it important in helping cancer cells survive therapy?
Metabolic reprogramming is a process in which cancer cells change/alter how they produce and utilize energy and build cellular materials that shift from normal metabolism to fuel rapid growth. To induce metabolic reprogramming, cancer cells exhibit changes in the genome, epigenome, proteome and metabolome. These cells use alternative fuels such as fatty acids and glutamine to maintain energy levels even under stress. Metabolic reprogramming helps cancer cells resist cisplatin. It does this by adjusting the antioxidant defense system of cells to overcome and neutralize drug-induced damage to cells, increasing the DNA repair capacity of cells, decreasing cisplatin import and increasing drug efflux. Thus, metabolic reprogramming helps cancer cells survive and continue growing. Thus, targeting metabolic reprogramming may be used as an approach against cancer cells to improve therapeutic outcomes.
Your study highlights the role of PDKs. Can you explain what these molecules do and why they are so important in cancer resistance?
Pyruvate dehydrogenase kinase (PDK) comprises four members (PDK1–4). They function as metabolic regulators by controlling the function and activity of the pyruvate dehydrogenase complex (PDC). These kinases phosphorylate PDC to inhibit processes that convert pyruvate into acetyl-CoA, preventing its entry into the TCA cycle and mitochondrial respiration. As a result, cells undergo lactic acid fermentation even in the presence of oxygen, a phenomenon known as the Warburg effect. In cancer, the overexpression of different members of PDK has been shown to activate oncogenic signaling, notably cell survival pathways and mitochondrial targeting. Accordingly, the PDK family has become an important treatment target. Blocking these kinases can restore mitochondrial oxidative function and improve the pro-apoptotic effects of chemotherapy drugs. In cervical cancer, we noted that the chromosome 14 miRNA cluster targeted PDK3. We detected reduced expression of the chromosome 14 miRNA cluster and increased expression of PDK3, which correlated with the reduced ability of cisplatin to kill cervical cancer cells. Restoration of the chromosome 14 miRNA cluster reduced PDK3 expression and, in turn, sensitized the cervical cancer cells to cisplatin by enhancing their cell-killing ability.
One key idea is that cancer cells shift how they produce energy. How does this shift help them escape the effects of chemotherapy?
Metabolic reprogramming allows cancer cells to escape cisplatin-induced cell death. Cisplatin kills cells by inducing extensive DNA damage. Cisplatin-resistant cells modify metabolism to generate a surplus of NADPH and glutathione. By binding to cisplatin, glutathione deactivates it to reduce its cytotoxic effect. Scavenging of ROS generated by cisplatin by NADPH is another route to escape from cytotoxicity. A shift toward increased glycolysis and fatty acid oxidation provides a high-energy reservoir of ATP and nucleotide precursors and promotes enhanced DNA repair. By modifying the way they produce energy, cancer cells ensure that they have enough biosynthetic resources to survive. They proliferate and grow even in the presence of toxins such as cisplatin.
How can targeting these metabolic pathways improve cancer treatment outcomes in the future?
This is the most exciting implication. If loss of the chromosome 14 miRNA cluster and subsequent PDK3 upregulation drive cisplatin resistance, then we have two complementary therapeutic strategies. We could administer artificial mimics of the deleted chromosome 14 miRNAs to reduce the expression of PDK3. Another possibility would be to target the kinase directly through inhibition by small molecules to reduce its activity. With a combination approach, we could first pretreat resistant tumors with mimics of chromosome 14 miRNAs or PDK3 inhibitors, effectively inducing mitochondrial metabolism and ROS generation and allowing apoptosis again. The sensitized cells can ultimately be treated with cisplatin for better outcomes. In our preclinical study, restoring the chromosome 14 miRNA cluster or inhibiting PDK3 pharmacologically sensitized resistant tumor cells to cisplatin. Overall, targeting this axis is a promising avenue for reversing resistance irrespective of the genetic profile of the tumor and may improve survival.
What are the greatest challenges researchers still face in translating this knowledge into real therapies for patients?
There are still several obstacles to overcome. First, there is the issue of delivery. The miRNA mimics are highly unstable and must be transported to target cells without being degraded. This can be overcome by using liposomes or viral vectors that have shown promise but have not been utilized consistently. Second, the existing PDK inhibitors are nonselective and inhibit all the isoforms. The development of isoform-specific inhibitors is thus highly desired. Third, metabolic redundancy is present. Cancer cells are adaptive, and if we target one metabolic pathway, such as the PDK3 axis, then they may adapt and find other ways to sustain themselves. Hence, an approach should be devised to kill these cells before they adapt to another pathway for survival. Fourth, identifying people who will benefit from targeting the chromosome 14 miRNA cluster-PDK3 axis is important.
What is the biggest message or conclusion from your research on cancer resistance?
Perhaps the most important conceptual shift from our work is that cancer resistance is not fixed. It is a dynamic state shaped by noncoding RNA regulation and metabolic adaptation. Rather than asking, “Which mutation causes resistance?”, we should ask, “Which regulatory and metabolic pathways stabilize resistance, and how can we destabilize them?” This perspective connects molecular events (loss of the chromosome 14 miRNA cluster → PDK3 upregulation → metabolic reprogramming) with clinical outcomes (chemotherapy failure). It also opens new avenues not only for cisplatin but also for other DNA-damaging drugs, such as carboplatin and oxaliplatin.
We are in the process of understanding the noncoding RNA-metabolic architecture of chemoresistance. Future advances may allow us to map miRNA and PDK3 expression profiles from patient biopsies, design tumor-specific miRNA mimics, or even predict resistance before treatment begins. In my view, the next frontier in oncology lies not only in sequencing cancer genomes but also in decoding the regulatory logic that allows some cells to survive while others die. In the end, cancer is not governed by mutations alone. It is governed by RNA networks, metabolism, adaptation, and the quiet resilience of a cell that has learned to rewire its own engine.










{kind=link}