
Many people use tobacco for decades without developing oral cancer, while others develop it much sooner. What inspired you to investigate the role of genetics in this striking difference?
This question arises from a common observation in society. While tobacco is the major cause of oral cancer, not everyone who uses tobacco develops the disease. Some individuals consume tobacco for decades without developing any high-risk oral lesions, whereas others develop oral cancer after a relatively short period of exposure. This suggests that factors beyond tobacco itself influence cancer risk. Our study focused on one of these key factors genetic susceptibility, which determines how effectively an individual’s body repairs damage caused by carcinogens.
In simple terms, what is genetic susceptibility, and why can two people with similar tobacco and/or alcohol habits have very different risks of developing oral cancer?
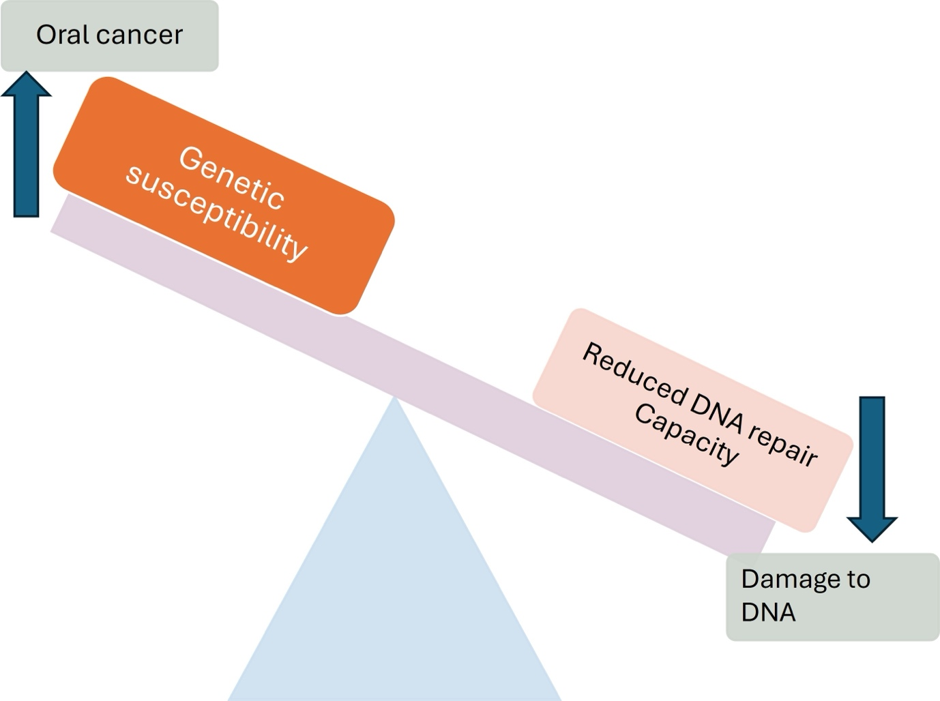
Every individual’s body has a natural ability to repair damage caused by harmful substances such as tobacco and alcohol. When this repair system works efficiently, damaged cells can be repaired or eliminated. However, if this protective capacity is reduced because of inherited genetic differences, DNA damage accumulates over time, increasing the risk of oral cancer. Genetic susceptibility is inversely proportional to an individual’s inherent capacity to repair DNA damage caused by various carcinogens. It means that if repair capacity is reduced or not functioning properly, the genetic susceptibility to developing cancer increases. Processes such as DNA repair, programmed cell death (apoptosis), immune surveillance, detoxification, and elimination of carcinogens all contribute to protecting the body, but their efficiency varies from person to person.
Your study identified several genes, including TP53, CASP8, HIF, DEC1, MTNR1B, and CYP1A1. What roles do these genes play, and why are they important in oral cancer?
Our analysis showed that variations (polymorphisms) in several genes are significantly associated with oral squamous cell carcinoma in people exposed to tobacco and alcohol. TP53, often called the “guardian of the genome,” prevents damaged cells from multiplying. CASP8 helps remove abnormal cells through programmed cell death. HIF regulates how cells respond to low oxygen conditions, while DEC1 participates in immune regulation. MTNR1B plays a role in physiological processes such as circadian rhythm regulation. Among these, CYP1A1 showed particularly strong associations in the Indian population because it activates tobacco-related chemicals into highly reactive compounds that can damage DNA and promote cancer development.
Your analysis found particularly strong associations in Asian populations, especially India, China, and Taiwan. Why might these populations be at higher risk?
Our study found higher odds of oral cancer-associated genetic polymorphisms in Asian populations than in many other populations. This increased susceptibility is likely due to a combination of inherited genetic factors and environmental exposures. In addition, tobacco products are widely cultivated and readily available in many Asian countries, increasing exposure from an early age. Therefore, both genetic susceptibility and environmental factors together contribute to the higher burden of oral cancer in these populations.
What is the most important message from your study for the public, particularly regarding tobacco use and individual cancer risk?
The most important message is that no one knows their own genetic susceptibility. Every individual has a different ability to repair DNA damage caused by carcinogens. Therefore, it is a mistake to assume that tobacco is safe simply because someone else has used it for many years without developing cancer. Genetics differs from person to person, and tobacco remains a proven carcinogen. The safest approach is to avoid tobacco altogether rather than relying on comparisons with others.
What should future research focus on in the area of genetic susceptibility to oral cancer?
Several important questions remain unanswered. More studies are needed to understand the hereditary contribution to oral cancer, particularly through large familial studies. Future research should also investigate how genetic susceptibility varies across different geographical regions and ethnic groups, helping identify high-risk genes in specific populations. Such studies will improve our understanding of why oral cancer prevalence differs worldwide and may eventually support more personalized approaches to prevention and risk assessment.










{kind=link}