
Glucagon-like peptide-1 receptor agonists, or GLP-1 RAs, have rapidly reshaped the treatment of type 2 diabetes and obesity. Medicines such as semaglutide are no longer niche therapies used only by specialists; they are becoming part of mainstream care because they can improve blood sugar control, reduce body weight, and lower cardiovascular risk. For many patients, that is a remarkable therapeutic advance. But as these drugs move from specialist clinics into wider real-world use, a new question has gained urgency: what are we learning about their effects on the eye?
The answer, at least for now, is nuanced. Most people taking GLP-1 medicines will never develop a serious eye complication, and the current evidence does not support abandoning these highly effective drugs. But pharmacovigilance data, trials, and case reports suggest that rare visual adverse events deserve closer attention. Two patterns stand out. One is worsening of diabetic retinopathy in some patients with diabetes, especially when blood glucose improves very rapidly. The other is rare optic nerve injury such as non-arteritic anterior ischemic optic neuropathy, or NAION, which can cause sudden vision loss and may leave permanent disability. Importantly, optic nerve events have been reported not only in diabetes, but also in some people using GLP-1 medicines for obesity alone.
That is why the issue now matters beyond ophthalmology. In 2025, the European Medicines Agency’s safety committee concluded that semaglutide should carry updated product information to reflect non-arteritic anterior ischemic optic neuropathy, or NAION, as a very rare side effect, with a frequency of up to about 1 in 10,000 treated people. The World Health Organization similarly issued a safety alert highlighting the seriousness of the condition and the need for continued vigilance. These actions do not imply that the drug is broadly unsafe. Rather, they signal an important shift in clinical thinking: as use expands, rare harms that were once difficult to detect become part of responsible prescribing and patient counselling.
These signals do not all reflect the same mechanism. Diabetic retinopathy worsening appears linked mainly to the speed and magnitude of glucose lowering in patients who already have retinal disease. Optic nerve events raise different questions about vascular susceptibility, anatomy, and whether semaglutide may act as one contributor among several in a small, predisposed subgroup. In other words, this is not one eye problem but two distinct clinical concerns in two different types of patients.
Two Distinct Eye-Safety Signals
Diabetic retinopathy progression was the first ocular safety signal to attract attention. In the SUSTAIN-6 trial, semaglutide was associated with more diabetic retinopathy complications than placebo, roughly 3.0% versus 1.8%. Later analyses suggested that the excess risk was concentrated largely in patients who already had retinopathy, had poor glycaemic control at baseline, and then experienced a marked early fall in HbA1c. That pattern fits the familiar phenomenon of “early worsening,” in which rapid correction of longstanding hyperglycaemia can transiently aggravate retinal disease before longer-term benefit emerges.
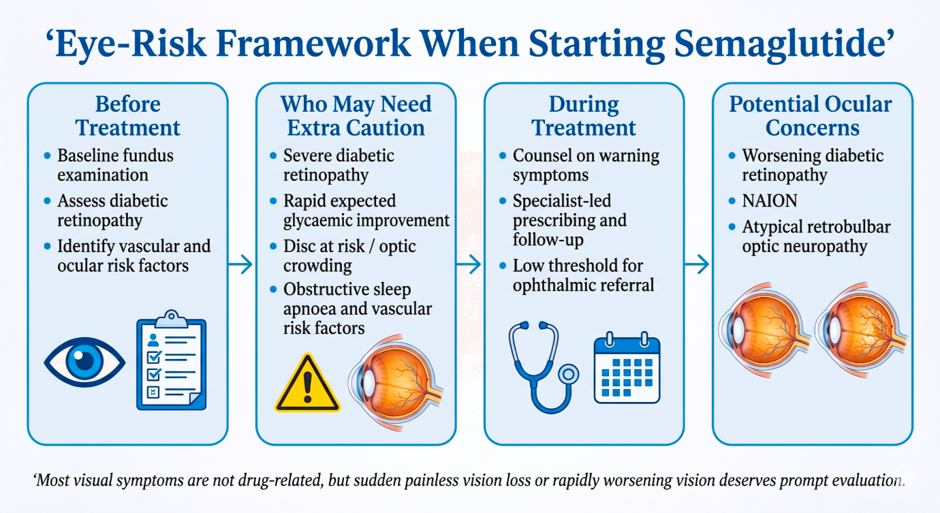
The practical lesson is not to avoid semaglutide in all patients with diabetes, but to identify those who may need closer monitoring when treatment starts. A recent retinal evaluation, awareness of baseline retinopathy status, and caution against pursuing very rapid metabolic change in vulnerable patients may all help reduce avoidable harm. Similar signals have not been consistently reproduced across most other semaglutide trials or across the GLP-1 class as a whole, suggesting a context-dependent risk rather than a universal toxic effect on the retina.
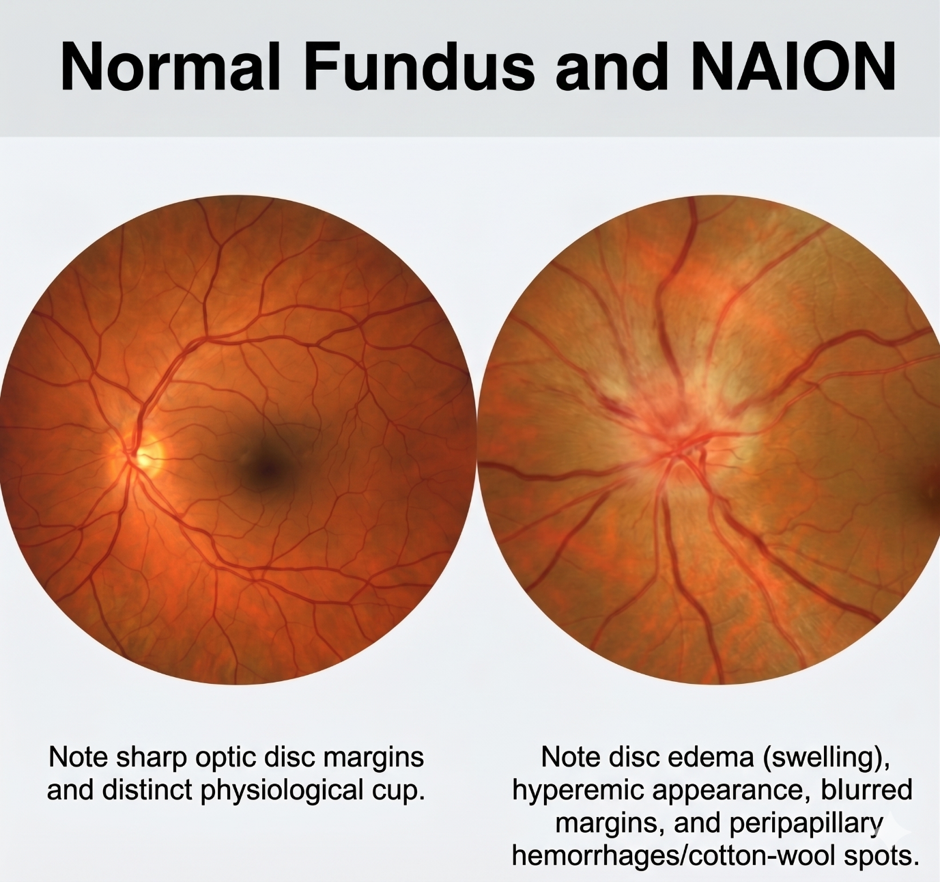
Optic nerve disorders, especially NAION, are the newer concern. NAION is a sudden loss of blood supply to the optic nerve that typically causes painless vision loss in one eye. It already occurs more often in people with diabetes, hypertension, dyslipidaemia, and obstructive sleep apnoea, which complicates interpretation because many people prescribed semaglutide carry the same background risks. Even so, large studies have suggested that semaglutide exposure may be associated with a higher incidence of NAION than expected. The absolute risk remains low, but the seriousness of the outcome has made this a major pharmacovigilance issue.
Many patients who develop NAION have a so-called “disc at risk”: a small, crowded optic nerve head with a low cup-to-disc ratio. In simple terms, there is less structural space within the disc, so even modest swelling may further compromise local blood flow and axonal transport. This helps explain why NAION can seem unpredictable: two patients may share similar vascular risk factors, yet the one with an anatomically crowded disc may be more vulnerable to a visual catastrophe. If the drug-associated signal is real, it is likely to affect only a very small subset of exposed patients with this kind of predisposition.
Recent regulatory action has moved this concern beyond isolated case reports. The EMA concluded that NAION should be listed as a very rare adverse effect of semaglutide, and the WHO likewise highlighted the need for continued vigilance. That does not mean most patients face meaningful visual danger. It means a rare event with potentially irreversible consequences has been observed consistently enough to deserve warning and recognition when symptoms occur.
Why Might These Problems Occur?
The biology is still being worked out. In diabetic retinopathy, the explanation is relatively familiar: rapid correction of long-standing hyperglycaemia can temporarily worsen pre-existing retinal disease. In optic neuropathy, the mechanism is less certain. Semaglutide may not directly damage the optic nerve, but could interact with pre-existing vascular vulnerability, sleep-apnoea-related risk, haemodynamic shifts, or disc anatomy in a small subgroup of susceptible patients.
The most realistic model is therefore one of convergence rather than a simple one-drug, one-effect explanation. Vascular disease, optic disc crowding, blood-pressure fluctuations, and treatment-related change may all matter at once. Our own recent experience reinforces that point. To our knowledge, this appears to be the first reported case from India of semaglutide-associated atypical retrobulbar optic neuropathy. We reported a young adult with obesity, obstructive sleep apnoea, and prediabetes who developed acute, painless, asymmetric bilateral visual dysfunction shortly after semaglutide dose escalation. The picture was unusual: there was no optic disc edema, imaging was unremarkable, and visual testing suggested a retrobulbar optic neuropathy with overlapping ischemic and demyelinating features rather than typical NAION. Because the presentation did not fit neatly into a classical syndrome, it serves as a reminder that potential semaglutide-related visual side effects may extend beyond the usual textbook description. That is exactly why clinicians should not wait for a perfect diagnostic label before taking new visual symptoms seriously.
What Should Patients and Clinicians Watch For?
Most visual complaints in diabetic or non-diabetic individuals with obesity who are receiving semaglutide or other GLP-1 receptor agonists will not be attributable to the medication itself. Even so, sudden, painless vision loss, new dimming in one eye, a dark patch in the field of view, or rapidly worsening eyesight deserves prompt evaluation. A baseline fundus examination before starting treatment is highly recommended, especially in patients with diabetes or other ocular risk factors. In diabetic patients, it can identify severe diabetic retinopathy that may be at risk of worsening if glycaemic improvement is rapid; where such retinopathy is present, it should ideally be stabilized and appropriate ophthalmic treatment initiated before semaglutide is started. It may also reveal a low cup-to-disc ratio or optic disc crowding, which could suggest a “disc at risk” in patients vulnerable to NAION. In such patients, counselling should be individualized and should include discussion that this anatomy may represent a predisposing factor, even though the absolute risk remains low and a baseline fundus examination cannot reliably predict who will or will not develop NAION or atypical retrobulbar optic neuropathy. At the same time, clinicians should remember that NAION and retrobulbar optic neuropathy can still occur even when the fundus appears normal, so a normal baseline examination should not create false reassurance.
These Are Not “Take-and-Forget” Medicines
None of this changes the fact that semaglutide and related GLP-1 medicines are major therapeutic advances. The challenge is not whether they should be used, but how they should be used well. These drugs are better understood as structured therapies that require counselling, dose-escalation planning, and attention to adverse effects across multiple organ systems. The eye has now entered that conversation as an area where rare but meaningful complications may occur.
The Indian context makes this especially important. When a powerful drug suddenly becomes cheap and widely available, it can encourage indiscriminate prescribing, especially in busy general practice settings where clinicians may not always have the time, specialist expertise, or systems needed for close follow-up. Many prescribers may also lack ready access to the ophthalmic evaluation or diagnostic setup required to investigate new visual symptoms in depth. In such circumstances, rare complications can be missed, delayed, or attributed to more familiar causes unless the possibility is actively considered. Wider access should therefore be matched by better counselling, clearer referral pathways, and a lower threshold for ophthalmic review when symptoms appear.
That does not mean every patient needs intensive ophthalmic surveillance. It means prescribers should be selective and practical: know baseline retinopathy status in people with diabetes, discuss warning symptoms clearly, and maintain a lower threshold for review in patients with vascular risk factors, obstructive sleep apnoea, or unexplained prior visual episodes. Given not only the potential for visual adverse effects but also other important complications of treatment, prescribing should ideally remain with specialists such as endocrinologists and experienced physicians who are better equipped to counsel patients, titrate therapy appropriately, and arrange timely follow-up when problems arise.
There is also a pharmacovigilance lesson here. Rare adverse effects become visible only when clinicians notice them, investigate them, and report them. As GLP-1 medicines spread across endocrinology, obesity practice, and general medicine, awareness will determine whether important signals are recognized early or lost in everyday prescribing. In that sense, the semaglutide-eye story is not only about one drug, but about how modern therapeutics should be introduced responsibly when their benefits are large and their rare complications may be serious.
So what are we learning? We are learning that the eye belongs in the safety conversation around weight-loss medicines, not because these drugs are broadly dangerous, but because rare complications become visible only after widespread use. We are learning that diabetic retinopathy worsening and optic neuropathy are not the same problem and should not be discussed as though they are. And we are learning that a low absolute risk does not remove responsibility when the consequence may be permanent loss of vision. Semaglutide and related GLP-1 therapies remain high-impact drugs with real public-health potential. The task now is to pair wider access with better counselling, selective monitoring, and faster recognition of the uncommon patient whose first warning sign may come through the eye.










{kind=link}