
Breast cancer is the most terrifying nightmare for many women as they grow older. “Am I going to be affected even though nobody in my family has suffered from it so far?” “Why do some breast cancers never return after treatment while others recur quickly?” These are common questions that arise whenever breast cancer is discussed. Every two minutes, one woman is diagnosed with breast cancer in United States. In India, every four minutes, one woman is diagnosed with breast cancer in higher stage than USA. We now understand that some breast cancers are much harder to treat than others because breast cancer is not a single disease. It is a heterogeneous disease with different pathological classifications, clinicopathological stages, molecular biology profiles, treatment protocols and different survival patterns.
Many factors are extremely crucial in breast cancer management, beginning with age, co-morbidities, size of the tumour, whether it has reached nearby draining lymph nodes or spread to other organs like the lungs or bones, favourable histologic types, and low or high tumour grades, which are overall classified according to the World Health Organization (WHO) pTNM staging system. Whether a particular chemotherapy, targeted therapy, hormone therapy, or immunotherapy treatment should be given to a woman diagnosed with breast cancer depends exclusively on the expression or status of certain pivotal test results, as per the guidelines of the American Society of Clinical Oncology and the College of American Pathologists. These include Estrogen Receptor (ER), Progesterone Receptor (PR), and HER2/neu testing. From these reports, molecular subtypes can be derived, which have prognostic and predictive value. When ER and PR are positive but HER2/neu is negative with low cell division, the subtype is called Luminal A. On the other hand, when ER is positive, PR is positive, and HER2/neu may be positive or negative with high cell division, it is categorised as Luminal B. When both ER and PR are negative but HER2/neu is positive, the subtype is called HER2-enriched. Lastly, Triple Negative Breast Cancer (TNBC) is the subtype in which ER, PR, and HER2/neu are all negative.
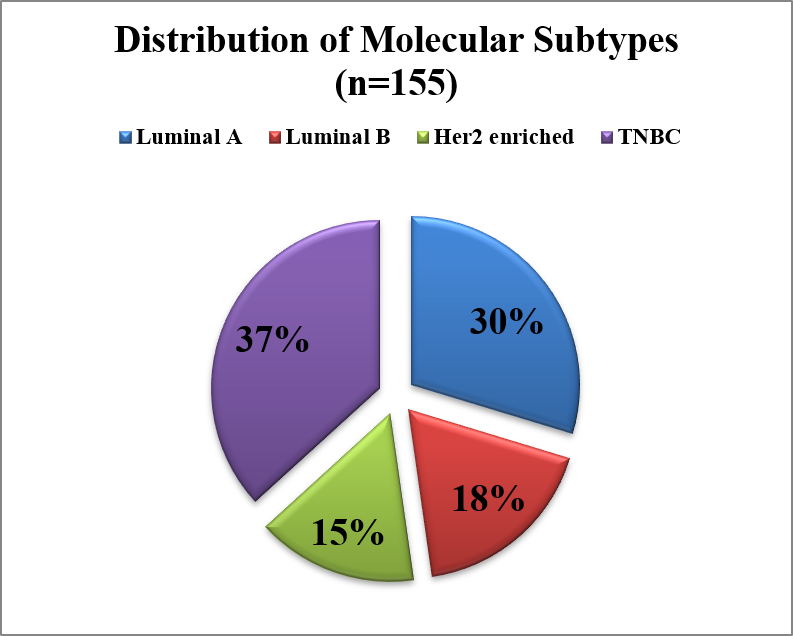
Luminal A molecular subtype of breast cancer is known for its excellent prognosis, with a 5-year survival rate of 95%. Luminal B is slightly more aggressive than Luminal A and also depends on whether HER2/neu is positive or negative. Luminal A and B are both eligible for treatment with anti-hormone receptor therapy. HER2-positive breast cancers are known for their aggressiveness, but they can be treated with targeted therapies like trastuzumab or pertuzumab. TNBC is the subtype that does not have any specific anti-estrogen or anti-HER2/neu therapy option, making it highly challenging to treat, and it is likely to have a poorer treatment outcome, with nearly 50% survival in contrast to Luminal A.
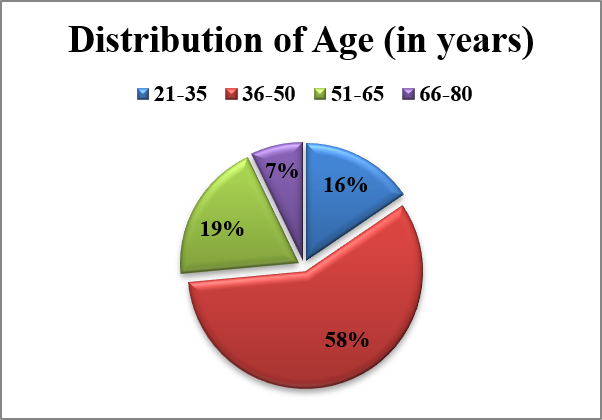
Unlike the Luminal A subtype, which is predominantly seen in studies from the USA and Europe, studies from Northeast India have shown that Triple-Negative Breast Cancer (TNBC) is the most common molecular subtype among breast cancer patients, followed by Luminal A, Luminal B, and HER2-enriched tumours. Our recent study also validated that TNBC is highly prevalent, with nearly one in three women diagnosed with breast cancer likely to have the TNBC subtype, which is an aggressive form of the disease. According to Cancer Registry data from the Indian Council of Medical Research, Northeast India has one of the youngest cohorts of breast cancer patients, with an average age at diagnosis of 47 years compared to 54 years for Pan-India and 65 years in the USA. The TNBC molecular subtype showed a strong association with the younger age group. This partly explains why one out of every two women diagnosed with breast cancer in India dies within five years, with survival being even lower in Northeast India.
Our recent publication “Association between molecular subtypes of breast cancer and surgical margin status from Assam, India” investigated the challenge of achieving clearer surgical margins by surgeons during breast cancer surgery.
The goal of surgeons is to remove the entire tumour tissue while maintaining clear surgical margins so that there is no chance of recurrence from any leftover tumour cells. This can be determined by the analysis of surgical margins by pathologists. The presence of cancer cells at the margins indicates a positive margin, which increases the risk of cancer recurrence and is seen in a significant number of patients. Such a situation may require the patient to undergo another surgery.
Our study showed that HER2-enriched tumours had the highest rate of margin involvement, followed by Luminal A, Luminal B, and TNBC cases. Larger tumours and cancers that had spread to lymph nodes were also associated with a higher rate of positive margins. These findings suggest that aggressive tumour types and advanced disease can make surgery more difficult. Our study findings showed considerably large tumour sizes, with 57% of cases measuring 2–5 cm and 38% measuring more than 5 cm, which had direct implications for surgical margin status. Lymph node involvement was observed in 77% of cases, indicating that the cancer was locally advanced and had a direct impact on survival in this cohort. From these findings, the importance of early detection, molecular testing, and proper surgical planning to improve breast cancer treatment outcomes in the Northeast Indian population must be emphasized.
Surgery is an extremely crucial part of breast cancer management because accurate assessment of tumour margins during surgery remains a major concern. However, in our study population, nearly 90% of patients underwent full breast removal (modified radical mastectomy), and only 10% were suitable for breast-conserving surgery. Most patients required more extensive surgical procedures due to the larger tumour sizes at presentation. Hence, achieving a negative tumour margin remained a challenge. We were also curious to determine whether TNBC had any association with surgical margin clearance, as TNBC is highly prevalent in this region.
One important result from the study showed a strong predilection for positive surgical margins in patients with larger tumour sizes and the aggressive HER2-enriched molecular subtype. We initially believed that TNBC would have higher margin involvement; however, it showed the least positive margins, surprisingly. We hypothesised that the HER2/neu molecular subtype may exert normal or near-normal physicochemical properties within the tumour tissue, making it difficult for surgeons to differentiate tumour tissue from normal tissue during surgery. There is a possibility that different molecular subtypes produce varying degrees of stiffness, pressure, temperature, optical density, and other physical properties, which may influence how tumour and normal tissues feel during surgical assessment.
Positive tumour margin remained a significant risk factor, placing nearly one out of three women with breast cancer at risk of local recurrence, and it was seen most commonly in the HER2-enriched molecular subtype. TNBC was the largest molecular subtype category, presented at a younger age, and was likely to be associated with poor prognostic parameters, thereby leading to poorer survival. However, the chance of positive margins was less common in TNBC than in other subtypes, probably due to the characteristic physicochemical properties evoked by this molecular subtype, allowing better distinction between normal and tumour tissue. The future direction of this research would involve more stringent margin assessment using radiological methods and frozen section analysis during the intraoperative period to reduce the chances of positive margins, along with the option of neoadjuvant chemotherapy followed by modified radical mastectomy (MRM). Technological characterisation of tumours is important so that surgeons can more precisely predict tumour margins. There is a strong need for solutions that can reduce positive margins during breast cancer surgery by improving the differentiation of tumour tissue from normal tissue. Such innovative methodologies could help bridge the existing technological gap in distinguishing cancerous tissue from normal tissue and thereby reduce the likelihood of positive margin involvement during breast tissue analysis in both the preoperative and intraoperative phases.
Our group is also currently working on multimodal fabricated MEMS-based electrical sensor and piezoelectric micro-machined ultrasound transducers (pMUTs) probe development for accurate intra-operative assessment of tumor margins.
Acknowledgment: The author gratefully acknowledges the grant received from the Indian Council of Medical Research (ICMR), Government of India, and the Anusandhan National Research Foundation (ANRF) (formerly the Science and Engineering Research Board, SERB), Government of India, for funding the research activities related to this work.










{kind=link}